BLOG
LUMPS, BUMPS AND A MASS LESION ON YOUR VOCAL CORD
At the Pretoria Voice Clinic we see many patients presenting with lesions or growths on their vocal folds.
Their main presenting symptom are hoarseness or problems with their singing voice.
There is no concensus in the literature regarding the nomenclature of mass lesions on the vocal cords.
This is causing a lot of confusion for patients and doctors alike.
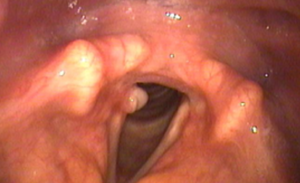
What lesion is this on your vocal cords?
Vocal cord nodules? or Vocal cord polyp with a secondary lesion on the other vocal cord? or Vocal cord cyst with a secondary lesion on the other vocal cord? or Bamboo nodules? or Fibrous lesion? or Granuloma? or Papilloma?
The answer is we do not always know.
The most common lesions that we see on vocal cords are haemorrhagic polyps, vocal cord nodules which are less frequently seen and vocal cord cysts.
Factors to take into consideration are:
History of voice usage is important.
Vocal overuse, professional voice users such as teachers. Phono traumatic event like shouting, screaming. History of tobacco and alcohol use.
Findings at flexible and rigid video laryngo stroboscopic features. Response to medical or proper voice therapy.
In some cases, the only diagnosis can be made by examination of the vocal cords and biopsy under direct examination under general anaesthetics in hospital.
Vocal Cord Nodules:
Vocal cord nodules are usually secondary to vocal overuse.
They are common in professional voice users such as teachers, singers, lawyers, judges, and preachers.
They are also common in children with vocal overuse.
Patients usually presents with hoarseness or having problems with their singing voice.
The best way in observing these lesions are either by rigid or flexible video laryngo stroboscopic evaluation done at our voice clinic.
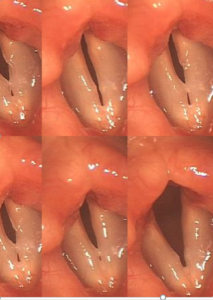
Video laryngo stroboscopic features of vocal nodules are:
They are fairly symmetric and present on both vocal cords. They have minimal influence on vocal fold vibration. It causes an hourglass configuration.
They usually respond well to voice therapy and rarely needed to be removed surgically.
Vocal Cord Polyps:
Vocal cord polyps are usually secondary to a phono traumatic event such as vocal misuse, such as screaming, yelling or during throat clearing.
Patients usually presents with hoarseness or having problems with their singing voice.
The best way in observing these lesions are either by rigid or flexible video laryngo stroboscopic evaluation done at our voice clinic.
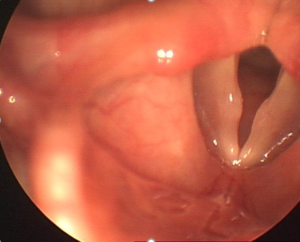
Video laryngo stroboscopic features of a vocal cord polyp:
They are usually present on only one vocal cord, there may be secondary lesions present on the other vocal cord. This might have the appearance which looks like bilateral vocal cord nodules.
They have minimal to moderate influence on vocal fold vibration.
It causes an hourglass configuration with glottic insufficiency. They usually respond well to good voice therapy alone and surgery is only indicated if they do not disappear on voice therapy alone and still causing hoarseness.
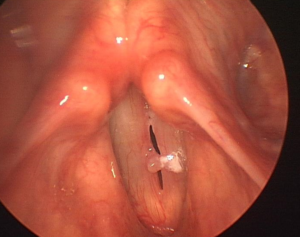
Vocal Cord Cysts:
Vocal cord cysts are sac like lesions filled with fluid usually located in the mid vocal fold.
There are usually two types of cyst, mucous retention cysts or keratin cysts. They can be congenital (born with it) or acquired.
Patients usually presents with hoarseness.
They can be either superficial in the vocal cord or deeper in the vocal ligament. The deeper ones affect the voice more than the superficial one and they are also more difficult to treat with poorer voice outcomes.
Polypoid Corditis (Reinke’s edema) are also saclike lesions on the vocal folds usually associated with smoking and vocal overuse.
Vocal Pseudo Cysts:

A vocal cord pseudo-cyst is a distinct cystic lesion on the mid free margin of the vocal fold.
They are usually secondary to a phono traumatic event such as vocal misuse, such as screaming, yelling or during throat clearing.
Some suggest that they form on the vocal cords due do vocal cord paralysis.
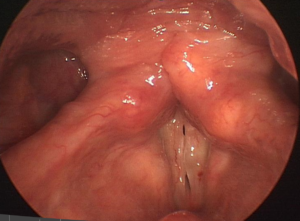
Vocal cord granuloma:
A vocal cord granuloma is an inflammatory mass usually located on the back part of one focal fold over the vocal process. They can also be present on both vocal folds.
A vocal cord granuloma is usually caused by phono- traumatic events such as vocal overuse.
They can also be caused by pressure, ulceration and inflammation caused by an endo tracheal tube passed through the vocal folds during surgery.
Laryngo pharyngeal reflux is a common contributing factor.
They usually respond well to medical therapy such as antibiotics, anti-reflux medication and good voice therapy.
In some cases, they can be quite refractive to treatment and need to be removed in the operation theatre. A biopsy is also needed if the lesion looks suspicious for cancer.
At our clinic we have successfully treated a few cases with surgical removal with a CO2 laser, intra-lesional cortisone and Botox to paralyse the vocal fold to reduce phono trauma.
Laryngeal papilloma:

Vocal cord papilloma are wart like growths on the vocal cords caused by the papilloma virus. They can occur in young children or in older adult people.
Young children usually present with hoarseness or upper airway obstruction.
Papillomatous lesions need to be removed if they are causing upper airway obstruction or suspicious of laryngeal cancer.
Several options of treatment are available:
– Frequent observation with video laryngo stroboscopy.
– Office flexible video laryngoscopy with blue laser (angiolytic laser) ablation.
– Micro-direct laryngoscopy in theatre, under general aneshetics and removal with cold steel, laser, micro-debridor or coblation.
Each technique has their own advantages and disadvantages.
the principle is to remove the papilloma without damaging the underlying lamina propria of the vocal folds. Damage to the underlying lamina propria of the vocal folds may lead to scar formation on the vocal folds with permanent hoarseness.
Laryngeal cancer

Cancerous lesions can also present as a mass on the vocal cords. Patients frequently presents with hoarseness, but only if the mass lesion is present on the vibrating part of the vocal cord.
When it occurs on the free mid margin of the vocal fold it frequently leads to voice problems. If it does not occur on the free edge, the patient might present much later.
Other symptoms might be throat irritation, throat clearing, swallowing problems and referred pain to the ears.
Vocal cord cancers are more frequent in patients using tobacco and alcohol. Treatment might include surgical removal or radiotherapy.